The Knowledge, Attitudes, and Practices Towards Prostate Cancer Screening Amongst Men Aged 18 and Above in Zambezi Region, Namibia.
Melody Buchane1, Jacob Sheehama2,4, Anna Alfeus3
1 Department of General Nursing, School of Health Sciences, Welwitchia University, Namibia
2Human, Biological and Translational Medical Sciences, School of Medicine, University of Namibia, Namibia
3Department of Public Health, School of Nursing and Public Health, University of Namibia 4TESA-University of Namibia , Trials of Excellence in Southern Africa Consortium
Dr Jacob Sheehama
The prevalence of prostate cancer (PCa) is a major health issue worldwide, including Namibia as a developing country. This study aimed to assess the level of knowledge, attitudes, and practices regarding screening of PCa among men aged 18 and above in Zambezi region. The study utilized a quantitative cross-sectional descriptive. A quantitative cross-sectional descriptive approach was used, with 391 men from all six constituencies of the Zambezi Region.
The results showed that respondents had moderate knowledge of prostate cancer and a generally positive attitude (49.9%) toward screening. However, this knowledge and attitude did not appear to influence actual screening practices, which were low at just 4.1%. The p-values of 0.927 and 0.692 are much greater than 0.05, indicating no statistically significant difference in the knowledge and attitude levels across the different constituencies. Regarding the practices, the variance of 0.3 was insignificant in performing a test. There was no relationship between knowledge and practices, attitudes and practices as indicated by the p-values. According to the data, significant positive associations (OR > 1, p-value < 0.05) were found in the 28-37 age group: OR = 3.05, p-value < 0.0001; 48-57 Age Group: OR = 2.71, p-value = 0.032; Single Individuals: OR = 3.12, p-value < 0.0001; Christianity: OR = 1.41, p-value = 0.009; and Employed: OR = 1.50, p-value = 0.112 (approaching significance)
Significant negative associations (OR < 1, p-value < 0.05), were found in married individuals: OR = 0.61, p-value = 0.009; Tertiary Education: OR = 0.64, p-value = 0.012; and Unemployed: OR = 0.37, p-value < 0.0001. Non-significant associations were found in groups such as the 58 and above age group, divorced individuals, primary-level, education, and other religions. These did not show statistically significant associations with attitudes toward screening of PCa. The infinity ORs (widowed, Islam) was due to no negative attitudes recorded in these groups, leading to an undefined result. The study concluded that knowledge and attitudes has no significant impact on screening practices therefore recommends further exploration into psychological factors and practice of PCa screening. In addition, a qualitative study to understand barriers to PCa screening and quantitative retrospective study on the analysis of the distribution of KAP within the six constituencies/ clusters of Zambezi region, Namibia.
Keywords: Prostate cancer, knowledge, attitudes, practices, screening.
Prostate cancer (PCa) is one of the most common cancers diagnosed in men across the globe (1). Data revealed that about 1/8 men will be diagnosed of PCa during their lifetime, with the risk increasing with age (2). PCa is a form of cancer that develops in the prostate gland, a small, walnut-shaped organ in the male reproductive system (3,4). Given the importance of these biochemical contributions, the prostate plays a crucial role in male fertility and reproduction, making it a significant organ in evolutionary biology (3). The exact cause of PCa remains unknown, however, various predisposing risk factors increase the likelihood of the development of the disease. These factors may include age, family history, race, and certain lifestyle choices, although ongoing research continues with the exploration of these associations.
Globally, healthcare systems are placing greater emphasis on public health interventions, such as screening programs, to decrease the severity of prostate cancer. However, disparities in knowledge, attitudes, and practices (KAP) towards the screening of PCa persist, especially in rural and underserved regions. These disparities are regarded to be influenced by several factors such as social and economic status, educational level, cultural beliefs, and access to healthcare services (7). Addressing these gaps is essential for reducing the incidence of advanced-stage prostate cancer and improving outcomes for men across various demographics (4). However, in this study, the researcher sought to assess the level of knowledge, attitudes, and practices (KAP) related to PCa screening among men in Zambezi region.
Through assessment of these factors, the study aimed at providing insights into the current state of awareness and engagement with screening of PCa in this region, which may inform future health interventions and educational programs. Furthermore, this study will serve as the primary data source for KAP in Zambezi region of Namibia. This chapter presents the background of the study, including the purpose, objectives, problem statement and significance of the study which set the foundation to understand the knowledge, attitudes, and practices of screening of PCa in Zambezi region. Furthermore, limitations and delimitation of the study, conceptual framework and definition of concepts will be discussed in this study.
Background of the study
Globally, prostate cancer is the most common cancer in men affecting 112 countries, with incidents varying from country to country (7,8). Furthermore, the data projections suggest a substantial increase in PCa cases in next years (3). In 2022, there were 1.467 million new cases of prostate cancer worldwide. Furthermore, globally, prostate cancer incidence and mortality rates vary significantly across the globe with Northern Europe having the highest incidence and Southern Africa the highest mortality rate in 2022 (9). Even though there have been an emerging of PCa development in young men and adolescence, PCa is more prominent in adults above 40 years of age (11,12). African men and those with a family history of PCa are most likely to develop PCa (4,13). Moreover, PCa is the second most frequent type of cancer in men, and it is the sixth most common cause of cancer-related fatalities among males, particularly among those of African descent, whose death rate is higher. PCa is the most common and leading cancer in men and the second leading cause deaths among the male gender in Namibia, representing 23.6% of all cancer cases (14,15). Furthermore, 68 PCa were recorded in Oshakati Intermediate Hospital of which 21% accounted for deaths in 2015 (14).
PCa is an escalating health issue in Africa, with incidence and mortality rates rising year on year. Africa recorded around 55744 deaths from PCa in 2022 alone (10). Age is a significant factor in relation to PCa, with PCa primarily affecting men over the age of 50 (7,16). As life expectancy in many African countries continues to improve, an increasing number of men are living in the age range where prostate cancer becomes more likely. This has inevitably led to a growing number of cases (17,18).
Cultural factors similarly play a significant role. In many African societies, there are deep-rooted taboos and misperceptions around reproductive health and masculinity. A study conducted in Nigeria highlighted that many men were reluctant to undergo prostate examinations due to fears surrounding the procedure and its perceived implications for their masculinity (20,21). This cultural reluctance to engage with healthcare services further delays diagnosis and treatment, leading to higher mortality rates. In addition, lack of medical aid schemes has been indirectly linked to lack of early screening of PCa hence germline PCa screening test are expensive (22). A study noted that obesity, coupled with these dietary changes, has been associated with higher PCa incidence and mortality rates in African populations (7).
The lack of widespread access to healthcare infrastructure is a further critical factor. Many African countries, particularly in rural areas, lack the resources for effective cancer prevention, diagnosis, and treatment (21,23). South Africa has more developed healthcare system, awareness of screening of PCa is moderate, particularly in urban centres (26).
Prostate cancer is a significant health issue in Namibia, with rising incidence and mortality rates, particularly due to late-stage diagnoses. According to the reports, (26)(3, prostate cancer accounts for 16.3% of all cancers diagnosed in men in the country, with around 332 new cases and 181 deaths in 2020 (33). Urban areas like Windhoek and Walvis Bay have better awareness and access to healthcare services, which allows for more opportunities for screening (33). However, even in these regions, cultural barriers and misconceptions about screening of PCa persist. In contrast, rural regions such as Oshana, Omusati, and Zambezi face more challenges, including limited access to healthcare infrastructure and lower awareness levels (34). Many men in these regions are hesitant to seek screening, influenced by cultural attitudes and a lack of understanding about the disease (33).
Namibia’s healthcare system is underdeveloped in many rural areas, contributing to the high number of late-stage diagnoses (20). In northern and southern regions, including Kavango and Karas, cultural beliefs and financial constraints further reduce participation in screening of PCa. Public health campaigns have progressed in urban centres, but rural areas remain underserved. Studies in these regions indicate that traditional beliefs and fear of medical procedures limit men’s engagement with formal healthcare (33). Addressing these disparities will require targeted efforts to improve healthcare access, increase public awareness, and reduce cultural barriers to screening of PCa across the country. There is a gap in the publication of PCa statistics in Zambezi region, Namibia, limiting the background of this study in the specified region. Katima Mulilo State Hospital (KMSH) Zambezi Region, which accounts for 25% of mortalities and incidences as per the KMSH Zambezi Region Inpatient and Outpatient Register 2021.
During clinical practices in the outpatient department in Katima Mulilo state hospital, in Zambezi region Namibia, the researcher observed an increased number of patients diagnosed with PCa stage two to three, who turned up for follow-up, some for referrals to Windhoek central hospital, one of the referral Hospitals in Namibia with oncology services which is 1200 kilometers away from Katima Mulilo, Zambezi region.
In the Zambezi region, the burden of prostate cancer is compounded by low screening rates, which hinder early detection and timely intervention. The researcher further observed that, there are no screening services in the outpatient department and clinics in Zambezi region, However, WHO recommends that men above the age of 40-year-old should undergo prostate cancer screening every after 12 months (7). The burden to the health care system, an increase in mortality without a reflection on published information, and without a better reflection of Men’s KAP regarding PCa screening triggered the researcher to conduct this study regarding the knowledge, attitudes, and practices towards screening for PCa among men in Zambezi region, Namibia.
Specific objectives of the Study
The purpose of this study was to assess the level of knowledge, attitudes, and practices towards PCa screening among-st men 18 and above in the Zambezi region, Namibia.
Significance of the study
The findings of this study provided valuable insights to the Ministry of Health and Social Services by establishing a scientific baseline of men’s knowledge, attitudes, and screening practices for prostate cancer in the Zambezi region. By identifying specific gaps in these areas, the study inform the development of targeted intervention strategies aimed at improving prostate cancer awareness and screening rates.
Lastly, the study has had a positive impact on the Respondents by enhancing their awareness and understanding of prostate cancer, potentially influencing their health behaviours and attitudes towards screening in the future.
Limitations and Delimitation of the study
Some respondents refused to participate to the study, however, ethical rules were abided to. Such respondents were not forced to participate rather excluded from the study. However, information regarding PCa was provided upon request. The researcher explained the importance of the study in the introductory phase of informed consent for generativity of accurate information.
The study specifically focused on the Zambezi region in Namibia. While the findings provided insights into knowledge, attitudes, and practices among men in this region, they may not have been generalisable to other regions in Namibia. The study boundaries were adult men aged 18 years old and above in the Zambezi region of Namibia.
This chapter discussed the research method, and the research design the researcher used in the study. Research method is the organized plan for conducting research. It encompasses the tools, techniques, and procedures used to collect and analyses data. A research design is a framework or blueprint for conducting the research. It outlines how the research will be conducted, including how data will be collected, measured, and analyzed. The research design ensures that the study was designed to address the problem identified by the study. It provides a logical sequence that connects the empirical data to the research questions and, ultimately, to the conclusions.
This study has employed a quantitative research approach. Furthermore, cross-sectional descriptive research designs were used to assess the knowledge, attitudes, and practices (KAP) regarding screening of PCa among the population in the Zambezi region, Namibia.
The cross-sectional component of the design meant that data collection occurred at a single point in time, providing a snapshot of the current state of KAP regarding screening of PCa. This is particularly useful for capturing information about the present situation in a specific population without requiring prolonged observation or follow-up. In this case, the cross-sectional method enabled the researchers to efficiently assess KAP on screening of PCa of the male population in the Zambezi region and report on the current trends without being influenced by changes that might occur over time.
The descriptive design used in this study was especially suitable given the research objective, which was to systematically describe the existing behaviour, knowledge levels, and attitudes toward screening of PCa. The goal was not to investigate cause-and-effect relationships or explore changes over time, in contrast to providing a clear picture of the status quo. This type of design is appropriate when the focus is on identifying and describing patterns and trends in behaviour (54), such as the proportion of individuals who are knowledgeable about screening methods, common perceptions of prostate cancer, and actual participation in screening programs.
A descriptive cross-sectional approach allowed the identification of prevalent trends, such as the percentage of individuals who were informed about screening of PCa options, the nature of prevailing attitudes toward the screening process (positive, neutral, or negative), and the actual practices, such as how frequently men in Zambezi region participated in screening programs.
The sampling strategy used in the study was designed to ensure that the findings could be generalised to the broader population in the Zambezi region, including the various constituencies within the region. By drawing a representative sample of the population, the research aimed to provide results that would reflect the overall knowledge, attitudes, and practices regarding screening of PCa across the entire community, ensuring that the insights gained could inform broader public health policies and initiatives targeted at improving screening of PCa in the area.
Population of the study and study setting
The population for this study comprised men aged 18 and above residing in the six constituencies of Zambezi region: Kabbe, Kongola, Katima Urban, Katima Rural, Linyanti, and Sibbinda.
The Zambezi Region, situated in the corner of Namibia at the north-eastern, is a geographically and culturally diverse area known for its rich natural resources and vibrant communities. The region comprises six constituencies: Kabbe North, Kabbe South, Kongola, Katima Urban, Katima Rural, Linyanti, and Sibbinda, with five of these being predominantly rural and one, Katima Urban, representing the only urban constituency (51). The population of the Zambezi Region is approximately 23,098 men (51).
The study conducted in the Zambezi Region covered all six constituencies, ensuring that the research captured a wide variety of environmental settings where men congregate, from May 2023 to June 2024. This was particularly important for reaching the diverse population, as men in rural areas are less likely to visit healthcare facilities routinely. As such, the study capitalised on existing social and community structures to reach a broad audience. Churches, Traditional authority gathering points, outpatient departments, clinics, Sports complex, villages offices complexes and other public venues where men regularly gather for recreational activities. These venues were ideal for capturing a large number of men who might otherwise be difficult to reach through conventional health outreach efforts.
Data Analysis
Data analysis includes categorising, ordering, manipulating and summarising the data, as well as describing those data in the meaningful terms (61). The data collected was verified before entering into the Statistical Package for the Social Sciences (SPSS) version 26 software which cleaned, categorised, and analysed the data. Descriptive statistics were used to present the data for easy analysis to determine the KAP for screening of PCa amongst men in the Zambezi region. The data analysis process involved several key steps to summarise, describe, and test the relationships between variables. First, descriptive statistics were employed to provide an overview of the dataset. This involved calculating and presenting means for continuous variables, allowing for the identification of central tendencies. Additionally, percentages and frequencies were calculated for categorical variables to summarise the distribution of responses across different categories, providing a clear snapshot of the characteristics of the respondents or responses.
Once the cross-tabulated data were obtained, the Chi-Square test of independence was applied. This statistical test determines whether there is a significant association between the categorical variables. Throughout the analysis, assumptions of the Chi-Square test, such as minimum expected frequency counts, were carefully checked to ensure the validity of the test results. Where necessary, adjustments were made to ensure the robustness of the analysis.
Ethical Considerations
The researcher obtained the ethical clearance certificate from the Human Research Ethical Committee (HREC) of the University of Namibia (UNAM), on 07 December 2022, Ethical clearance reference number DEC OSH 0029. Moreover, a formal approval from the Ministry of Health and Social Services and Zambezi regional governor, board and constitutional counsellors was granted. In line with ethical standards, the study adhered to four fundamental ethical principles: autonomy, beneficence and non-maleficence, and justice. The following principles were observed: autonomy, informed consent and transparency, Principle of Beneficence and Non-maleficence, Principle of Justice and Protection of Vulnerable Populations
Presentation Of Data
The results of the study shows, that the total of 393 questionnaires distributed, 391 respondents, yielding an impressive response rate of 99.5%. This high response rate reflects the Respondents’ engagement with the study and enhances the reliability and validity of the results. The chapter begins by detailing the socio-demographic characteristics of the respondents, which include age, education level, employment status, and other relevant background information that may influence their knowledge, attitudes, and practices regarding PCa screening. Following this, the analysis of the Respondents ‘ knowledge about PCa, examining their awareness of the disease, risk factors, symptoms, and available screening methods is presented. The chapter then explores the respondents’ attitudes toward PCa and its screening, assessing their perceptions, beliefs, and potential barriers that might affect their willingness to engage in screening practices. Finally, the chapter examines the practices of the respondents concerning PCa screening, focusing on whether they have undergone screening, their frequency of participation in such practices, and the reasons behind their decision to either engage or not engage in screening.
Demographic characteristics of respondents per constituency
This section presents the demographic data of the respondents per site, that is, Kabbe, Kongola, Linyanti, Katima Mulilo urban, Katima Mulilo rural and Sibbinda.
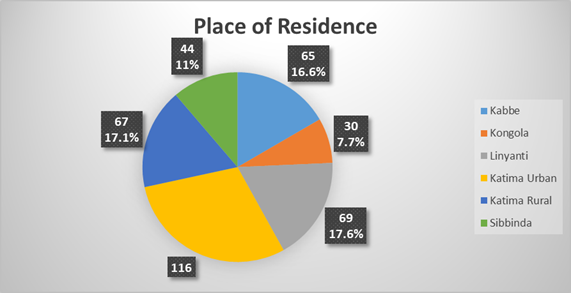
Figure 1: Respondents’ Place of Residence
Most respondents, n=116 (29.7%) are resident in Katima urban, followed by n=69 917.6%) from Linyanti. Those from Katima rural and Kabbe were 67 (17.1%) and 65(16.6%) respectively. Sibbinda had 44 (11%) respondents and only 30 (7.7%) Respondents came from Kongola.
The data shows that the majority of individuals across all age groups were unemployed covering up to 93% of the total and have no formal education tallying up to 89% , with 100% Christianity as their religion . In terms of marital status, most individuals aged 28-47 were married (55%), while the younger age group (18-27) has a mix of single and married individuals. Divorce is more common in the older age groups (48 and above) which is 86%, and there are a few cases of widowhood of 50% in the oldest group. A small number of individuals in the 18-27 age group had secondary or tertiary education, but this trend does not continue in older age groups. Employment status of 7% is very low across all age groups, with only a few individuals employed, mainly in the younger age group.
Table 2. Summary of Demographic Characteristics of the Respondents
| Characteristic | Frequency | Percentage (%) |
|---|---|---|
| Age Range (years) | ||
| 18–27 | 129 | 33.0 |
| 28–37 | 105 | 26.9 |
| 38–47 | 72 | 18.4 |
| 48–57 | 39 | 10.0 |
| ≥58 | 46 | 11.7 |
| Marital Status | ||
| Married | 129 | 33.0 |
| Single | 249 | 63.7 |
| Divorced | 10 | 2.5 |
| Widowed | 3 | 0.8 |
| Educational Level | ||
| No Formal Education | 63 | 16.2 |
| Primary Level | 26 | 6.6 |
| Secondary Level | 153 | 39.1 |
| Tertiary Level | 149 | 38.1 |
| Religion | ||
| Christianity | 370 | 94.8 |
| Islam | 3 | 0.6 |
| Others | 18 | 4.6 |
| Employment Status | ||
| Employed | 97 | 24.8 |
| Unemployed | 294 | 75.2 |
The above data presents the characteristics of Respondents. Most Respondents were between the age group of 18-27 (33%) years followed by those between 28-37 years (26.9%). Regarding marital status, 250 (63.9%) were single, 129 (33%) were married, 10 (2.5%) were divorced and only 3 (0.6%) were widowed. On the educational level, 153 (39.1%) have secondary level education, and those with tertiary education were 146 (38.1%). Respondents without formal education were 63 (16.2%) and those with primary school level education were 26 (6.6%). Christianity was the predominant religion with 370 (94.8%), other religions not specified, 18 (4.6%) and Islam had 3 (0.6%). Ninety-seven (24.8%) were employed while 294 (75.2%) were unemployed.
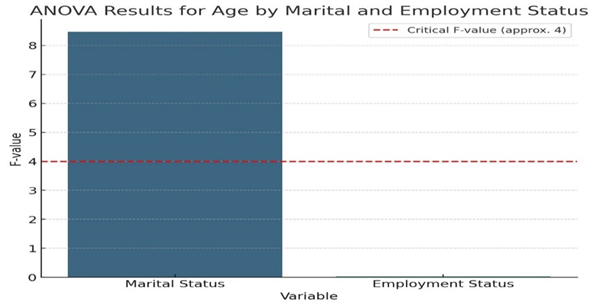
Figure 3: Analysis of the Age, Marital, and Employment status across constituencies
The F-values for each variable are shown, with a dashed line indicate an approximate critical F-value of 4. This highlights the significant effect of marital status on age (with an F-value of 8.47), while employment status has a negligible effect (F-value of 0.033).
Knowledge of Prostate Cancer
This section presents the respondent’s knowledge regarding prostate cancer.
The data reveals varying levels of awareness about prostate cancer across different age groups and constituencies. In Kabbe, 22 individuals (out of 65) across all age groups have heard of prostate cancer accounting for 34% of awareness, with the highest in the younger age groups (8 individuals each in 18-27 and 28-37) and no awareness among those aged 58 and above. Sibbinda shows lower awareness, with only 8 individuals (out of 44) aware with a percentage of 18%, particularly in the 28-37 age group (3 individuals). In Linyanti, 37 individuals (out of 69) have heard of prostate cancer accounting for 54%, with the highest awareness in the 28-37 age group (15 individuals), but a significant number (32 individuals) still do not know what it is. Katima Urban stands out with the highest awareness of 71%, where 82 individuals (out of 116) have heard of prostate cancer, particularly across all groups. In Katima Rural, 46 individuals (out of 67) are aware, with higher awareness in younger and middle-aged groups, but still 21 individuals remain unaware (31%) .In Kongola, only 8 individuals (out of 30) aware of prostate cancer accounting for 23% of awareness, similar to Sibbinda of 18%, with minimal awareness across all age groups. Overall, awareness tends to be higher in urban areas and among younger to middle-aged groups.
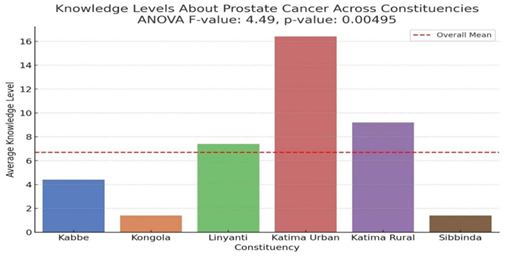
Figure 4: Analysis of respondent’s awareness of PCa across the constituencies
The F-value is 4.49 with a p-value of 0.00495. Since the p-value is less than 0.05, the results reject the null hypothesis and conclude that there is a statistically significant difference in awareness levels about PCa across the different constituencies suggesting that awareness of prostate cancer varies significantly between constituencies.
The respondents were required to indicate the source of information if they answered ‘yes’ to have heard about prostate cancer.
Table 3: Source of Information
| Source | Frequency | Percentage (%) |
| Health Care Providers | 52 | 25.7 |
| Media (TV, Radio) | 66 | 32.9 |
| Internet | 48 | 23.7 |
| Friends and Family | 28 | 13.9 |
| Other (Not specified) | 8 | 3.9 |
| Total | 202 | 100% |
The table summaries the sources of information about screening of PCa among respondents. Out of 391, 202 sources of information is displayed above, in exclusion of 189 who had never heard about PCa. The most common source is media (TV, Radio) at 32.9%, followed by health care providers (25.7%), the internet (23.7%), friends and family (13.9%), and other unspecified sources (3.9%).
Regarding early signs of PCa, painful ejaculation was recognised as an early warning sign by a significant number of respondents in Katima Urban (KU), with 14 respondents selecting this option. Conversely, ‘Don’t know’ was a common response in all constituencies, with Katima Urban (KU) having the highest number (27 respondents), indicating a notable gap in awareness regarding the symptoms of prostate cancer.
To analyse the knowledge levels across constituencies, a logistic regression model was used to model the probability of being knowledgeable based on constituency.
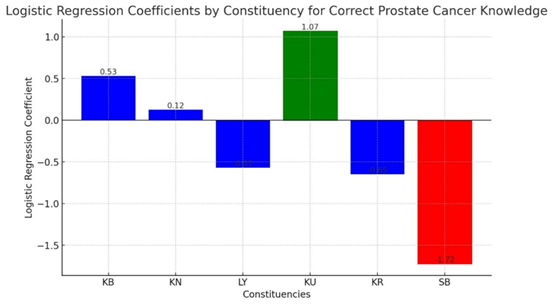
Figure 5: Logistic regression analysis of knowledge levels
Katima Urban (KU) has the highest positive coefficient (1.0678), indicating that respondents from Katima Urban are more likely to correctly identify PCa as prostate cancer compared to the baseline (the baseline constituency is not explicitly defined but is implied by the reference category, typically one of the other constituencies). Sibbinda (SB) has a strongly negative coefficient (-1.7225), indicating that respondents from Sibbinda are much less likely to identify prostate cancer compared to the baseline correctly. The other constituencies (KB, KN, LY, KR) have varying degrees of association with correct prostate cancer knowledge. The logistic regression model is statistically significant (as indicated by the LLR p-value), meaning that the differences in knowledge levels across constituencies are not due to random chance.
Attitudes towards PCa Screening
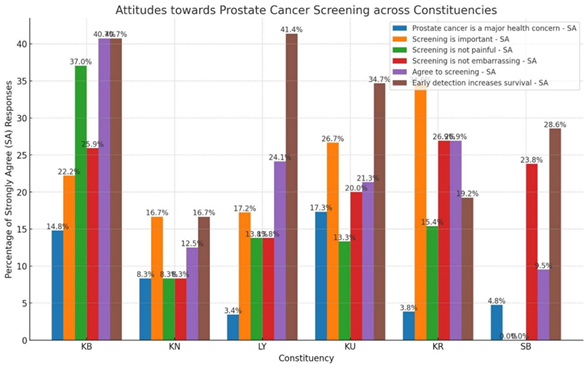
The bar graph comparing attitudes towards screening of PCa across urban and rural constituencies shows that Katima Urban (KU) consistently exhibits the highest levels of strong agreement (SA) across all categories. For example, 34.7% of respondents in KU strongly agree that early detection increases survival, compared to an average of 11.9% in rural constituencies. KU also leads in the belief that prostate cancer is a major health concern (17.3% SA) and in agreeing to go for screening if recommended (26.7% SA). In contrast, rural constituencies, particularly Sibbinda (SB) and Kongola (KN), show lower percentages, with SB having 0% SA for the importance of screening and only 4.8% SA in acknowledging prostate cancer as a major health concern.
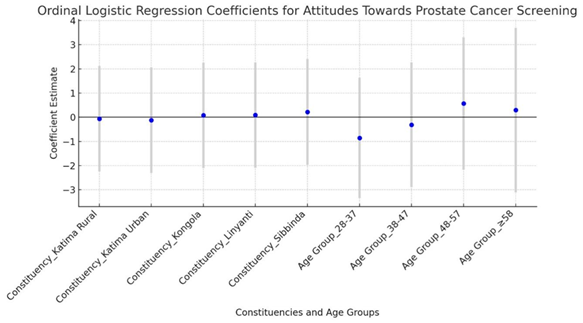
Figure 7: Ordinal logistic regression analysis for age and attitudes
Most of the coefficients are close to zero, indicating a lack of strong effect from the constituencies or age groups on the attitude levels. The ordinal logistic regression model suggests that neither constituency nor age group significantly impacts attitude levels towards screening of PCa in this dataset. The model had difficulty converging, as indicated by the convergence warnings, and the overall fit is relatively weak.
An ordinal logistic regression model was also used to analyse the relationship between level of education and attitude levels as displayed in the following Figure.

Figure 8: Relationship between educational level and attitudes towards PCa screening
The above figure shows that the positive coefficients (above zero) suggest that individuals in those categories have a higher attitude level towards screening of PCa. Tertiary education level has a notable positive coefficient, reinforcing the earlier observation that higher education is associated with more positive attitudes. The regression analysis indicates that the coefficients for all constituencies were not statistically significant. This suggests that, after controlling educational level, the constituency in which a person lives does not have a significant impact on their attitudes towards screening of PCa. While some constituencies, such as Katima Urban and Sibbinda, showed positive coefficients (indicating a potentially more positive attitude), the wide confidence intervals and lack of statistical significance cannot be confidently concluded that these constituencies differ meaningfully from others in terms of attitude.
Table 4: Attitude levels towards PCa
| Attitude Category | Number of Responses | Percentage of Total Responses |
| Positive Attitudes (Agree + Strongly Agree) | 195 | 49.9% |
| Negative Attitudes (Disagree + Strongly Disagree) | 94 | 24.0% |
| Neutral Attitudes (Neutral) | 102 | 26.1% |
| Total Responses | 391 | 100% |
The overall positive attitude level is 49.9%, and the overall negative attitude level is 24.0%.
Practices towards PCa Screening
The last section of the questionnaire required the respondents to answer questions regarding the practices towards PCa screening.
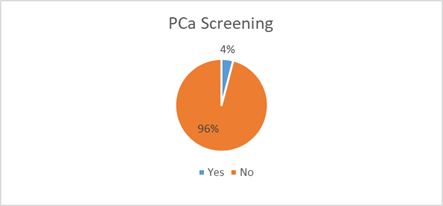
Figure 8: PCa Screening done
Only 16 (4%) respondents said they had done PCa screening with 375 (96%) never done PCa screening.
The frequency of the last prostate cancer (PCa) screening among respondents, shows that five individuals had their last screening within the past 3 to 5 months, two within the last 6 to 11 months, and nine had their screening 12 months or more ago.
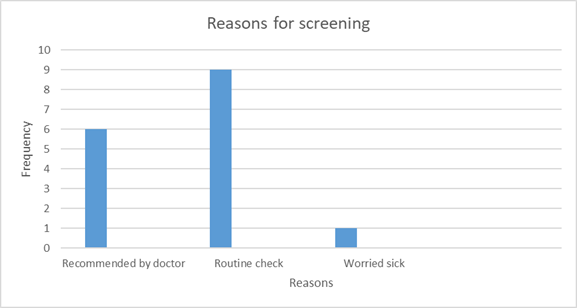
Figure 10: Reasons for Screening.
Nine respondents were screened as a routine check, 6 were recommended by their doctors and 1 was worried as they felt sick.

Figure 11: Barriers to PCa Screening
The bar chart illustrates the frequency of various barriers to accessing a particular service, likely related to healthcare, as reported by respondents. The most significant barrier, with a frequency of 203 accounting for 52%, is the unavailability of screening services at the clinic, indicating a critical gap in service provision. Lack of awareness follows, with 104 (27%) instances, suggesting that many individuals are not informed about the service or its importance. Cultural factors are also notable, with 81 respondents citing culture as a barrier with 21%. Fear of pain and the distance to the healthcare facility are also considerable obstacles, with frequencies of 66 and 45, respectively. The least cited barrier is the cost, with only 27 respondents (7%) considering the service to be expensive . This distribution highlights the importance of service availability and awareness in overcoming barriers to healthcare access.
The data reveals significant challenges and variations in screening of PCa practices across six constituencies, highlighting a generally low uptake of screening services, particularly in rural areas.
Table11: Analysis of KAP across constituencies’ summary table
| Category | F-Statistic | P-Value |
| Knowledge | 0.009 | 0.927 |
| Attitudes | 0.564 | 0.692 |
The p-values of 0.927 and 0.692 are much greater than 0.05, indicating no statistically significant difference in the knowledge and attitude levels (i.e., prostate cancer awareness) across the different constituencies. Regarding the practices, the variance of 0.3 was insignificant in performing a test.
In the table above, the Odds Ratio (OR) compares the odds of being in the higher knowledge (HK) group versus the lower knowledge (LK) group for each age category. An OR > 1 suggests that individuals in that age group are more likely to be in the HK group (higher knowledge) compared to the LK group (lower knowledge). An OR < 1 indicates that individuals in that age group are less likely to be in the HK group compared to the LK group. An OR close to 1 suggests no significant difference in knowledge between the two groups for that age category.
According to the data presented in the above table, significant positive associations (OR > 1, p-value < 0.05) were found in the 28-37 age group: OR = 3.05, p-value < 0.0001; 48-57 Age Group: OR = 2.71, p-value = 0.032; Single Individuals: OR = 3.12, p-value < 0.0001; Christianity: OR = 1.41, p-value = 0.009; and Employed: OR = 1.50, p-value = 0.112 (approaching significance)
Significant negative associations (OR < 1, p-value < 0.05), were found in married individuals: OR = 0.61, p-value = 0.009; Tertiary Education: OR = 0.64, p-value = 0.012; and Unemployed: OR = 0.37, p-value < 0.0001. Non-significant associations were found in groups such as the 58 and above age group, divorced individuals, primary-level, education, and other religions. These did not show statistically significant associations with attitudes toward screening of PCa. The infinity ORs (widowed, Islam) was due to no negative attitudes recorded in these groups, leading to an undefined result.
This study concluded that there is a significant relationship between knowledge and attitudes which means that individuals with know more about the screening of prostate cancer have positive attitudes toward it. However, this positive attitude does not necessarily translate into action, as the study found no significant relationship amongst attitudes and the actual practice of undergoing screening. Similarly, there is no significant relationship between knowledge and practices of PCa screening. The study also concludes that educational level is the most significant determinant of knowledge about screening of PCa, with higher education strongly linked to greater awareness.
The results showed that respondents had moderate knowledge of prostate cancer and a generally positive attitude (49.9%) toward screening. However, this knowledge and attitude did not appear to influence actual screening practices, which were low at just 4.1%. Statistical analysis (p-values of 0.927 of knowledge and 0.692 of attitudes) revealed no significant differences in knowledge and attitudes across constituencies. Additionally, the analysis showed no relationship between knowledge and screening practices and between attitudes and practices. However, there was a significant relationship between knowledge and attitudes. Education level was found to be significantly associated with knowledge, while other demographic factors showed no significant correlation. The study concluded that knowledge and attitudes alone do not significantly impact screening practices. It recommends further research into psychological factors influencing screening behavior, as well as a qualitative study to explore barriers to screening of PCa.